
Understanding Your Gleason Score: Why It Matters for Men with Prostate Cancer
When you first hear the words “Gleason Score,” it may sound technical or confusing. Understanding this simple number can help you take back control of your health and choices.
Knowing what your Gleason Score means can calm fears, guide your next steps, and help you discuss treatment options with clarity and confidence.
1. What Is the Gleason Score?
The Gleason Score is a system that describes how aggressive prostate cancer might be. Dr. Donald Gleason developed it more than 60 years ago, and it remains one of the most reliable ways to predict how a prostate cancer is likely to behave.
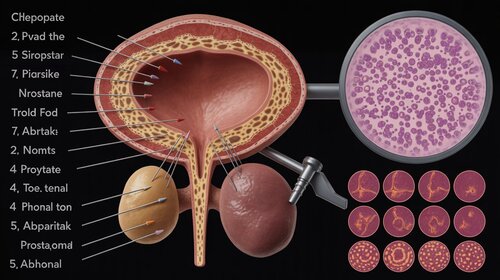
By studying the patterns of prostate cells under a microscope, doctors estimate whether the cancer is slow-growing or faster-moving.
Key points:
- It shows how likely your cancer is to grow or spread.
- It helps guide whether immediate treatment is needed or if careful monitoring is safe.
2. How the Gleason Score Is Calculated
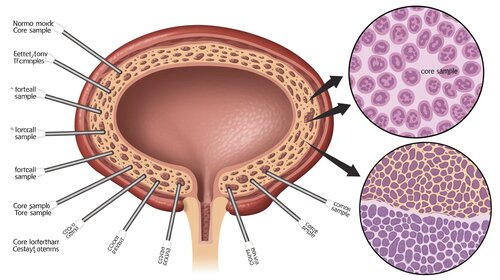
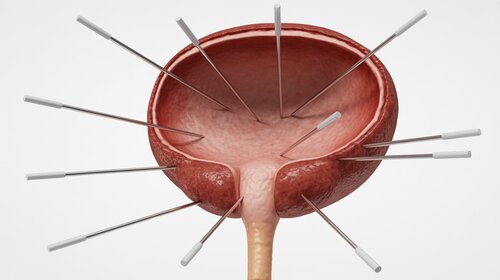
Your Gleason Score comes from a prostate biopsy. Small tissue samples are taken from different parts of your prostate. A pathologist examines these samples to see how much the cells differ from normal prostate tissue.
Grading overview:
- Grade 1 or 2: Cells look nearly normal. These are rarely used today.
- Grade 3: Cells look somewhat abnormal but remain organized.
- Grade 4: Cells look more irregular and less structured.
- Grade 5: Cells look very abnormal and are most likely to spread.
Your Gleason Score combines two grades: the most common pattern and the second most common pattern seen under the microscope.
Examples:
- Main pattern Grade 3 and next pattern Grade 4 gives a score of 3+4 = 7.
- Main pattern Grade 4 and next pattern Grade 3 gives a score of 4+3 = 7.
3. What Your Gleason Score Means
| Gleason Score | Risk Level | What It Means |
|---|---|---|
| 6 (3+3) | Low | Slow-growing and less likely to spread. |
| 7 (3+4) | Favorable Intermediate | Moderate risk and less aggressive. |
| 7 (4+3) | Unfavorable Intermediate | Moderate risk and more aggressive. |
| 8 (4+4, 3+5, 5+3) | High | More likely to grow and spread quickly. |
| 9–10 (4+5, 5+4, 5+5) | Very High | Very aggressive and more likely to spread. |
Should Gleason 6 Even Be Called Cancer?
An increasing number of respected urologists and pathologists now argue that a Gleason 6 (3+3) tumor should not even be classified as “cancer.” These cells typically stay confined to the prostate, rarely spread, and behave more like a benign condition than a life-threatening disease. Studies show that men with pure Gleason 6 lesions almost never die from prostate cancer, even without treatment.
Because of this, many experts are calling for a new term—such as “low malignant potential lesion”—to help reduce unnecessary fear and overtreatment. Understanding this perspective can help men approach their diagnosis with calm and confidence rather than panic.
4. Why the Difference Between 3+4 and 4+3 Matters
Even though both equal 7, the order matters. A 3+4 behaves more like a Grade 3 cancer, while a 4+3 behaves more like a Grade 4. The first number is the dominant pattern, and it has a strong influence on how the cancer acts overall.
- 3+4 = 7: Often less aggressive and sometimes safe to monitor with active surveillance.
- 4+3 = 7: Usually more aggressive and more likely to need treatment such as surgery or radiation.

5. How Understanding Your Gleason Score Empowers You
5.1 It Simplifies Decision-Making
Knowing your score helps you weigh choices. Men with low-risk prostate cancer, such as Gleason 6 or sometimes 3+4, can often choose active surveillance. Men with higher scores may consider earlier treatment.
5.2 It Replaces Fear with Facts
When you understand your score, you move from fear to focus. You can ask better questions, compare options, and take part in your care plan with confidence.
5.3 It Helps Prevent Unnecessary Treatment
Careful studies show that many men with low-risk prostate cancer live long and healthy lives without aggressive treatment. Avoiding unnecessary procedures protects quality of life and lowers the risk of side effects such as impotence or incontinence.
5.4 It Encourages Second Opinions
If your biopsy suggests a higher grade, a second pathologist's review is wise. In some cases, a second opinion changes the score and the treatment plan.

6. The Limitations of the Gleason Score, and How to Address Them
A prostate biopsy samples only a small part of the gland, often less than one percent. Higher-grade cancer can be missed. To improve accuracy, consider these options:
- MRI-targeted biopsy: Focuses on suspicious areas with better precision than a standard biopsy.
- Genomic testing: Looks for biological signals that show how likely your cancer is to grow or spread.
7. Key Questions to Ask Your Doctor
- How confident are you in my Gleason Score, and should I get a second opinion on the pathology?
- Does my score suggest that active surveillance is a safe option for me?
- What are the benefits and risks of immediate treatment for my score?
- Would an MRI or a genomic test give us a clearer picture of my cancer?
8. Conclusion: Knowledge Is Power
Your Gleason Score is more than a number. It is a guide that helps you move forward with steady confidence. Understanding it can reduce uncertainty, improve conversations with your care team, and help you protect both your health and your quality of life.
What We've Learned in This Chapter
- The Gleason Score describes how aggressive a prostate cancer might be.
- The two numbers in your score show the dominant and secondary patterns seen under the microscope.
- Your score guides whether monitoring or immediate treatment is more suitable.
- Second opinions, MRI-targeted biopsy, and genomic testing can refine the picture.

Action or Reflection Step
Write down your Gleason Score and bring it to your next appointment. Ask your doctor what each number means and whether MRI-targeted biopsy or genomic testing could help you make a clearer, calmer decision.
About the Author
Scott Oliver, 66, is living well with prostate cancer after dedicating more than 4,000 hours to researching the condition. His first goal is to help men reduce their risk of developing prostate cancer through proven lifestyle strategies.
When diagnosed, his mission is to help men avoid unnecessary prostate surgeries that can lead to devastating complications such as incontinence, bleeding, permanent impotence, and a loss of length.
Scott Oliver is not a doctor and does not offer medical advice; however, he is healthier and fitter than he has been in decades. Through his articles and videos, he shares hard-to-find, uncensored information on proven alternative therapies, effective fitness methods, and repurposed drugs, content that most doctors won’t mention and search engines suppress.
He is an accredited member of the National Writers Union (NWU) and the International Federation of Journalists (IFJ), the world’s largest organization of professional journalists. Scott is also the author of What If Cancer’s Best Defense Is Free? Sleep as a Defense Against Cancer: A Former Royal Marines Commando’s 4,000-Hour Research Roadmap, where he reveals how sleep repairs DNA, restores immunity, and strengthens the body’s natural defenses against cancer.
You can always contact Scott Oliver here with your questions and suggestions.
Scientific References and Notes
This article began with research, not opinion. Every conclusion is grounded in peer-reviewed journals, clinical-trial data, and expert analysis. As someone living well with prostate cancer, I combine that research with firsthand experience—translating credible science into clear, practical guidance for men and the women who love them, free from industry bias and medical jargon.
-
The Gleason Grading System: Past, Present, and Future
Explains how Dr. Donald Gleason's system became the global standard for assessing prostate cancer aggressiveness and how refinements improved its accuracy and reliability.
Source: Epstein JI, Human Pathology (2016).
-
Prostate Cancer Grade Group System: A More Accurate and User-Friendly Classification
Introduces the modern “Grade Group” system that simplifies Gleason scores into clearer clinical categories to guide treatment choices.
Source: Pierorazio PM et al., BJU International (2016).
-
Long-Term Outcomes of Active Surveillance for Prostate Cancer
Demonstrates that men with low-risk prostate cancer, particularly Gleason 6, can be safely monitored for many years with minimal disease-specific mortality.
Source: Klotz L et al., Journal of Clinical Oncology (2015).
-
MRI-Targeted Biopsy versus Standard Biopsy for Prostate Cancer Diagnosis
Finds that MRI-guided biopsy detects more clinically significant cancers and reduces over-diagnosis of low-grade disease compared with standard biopsy methods.
Source: Kasivisvanathan V et al., New England Journal of Medicine (2018).
-
Genomic Classifiers for Risk Stratification in Prostate Cancer
Shows that genomic tests provide additional prognostic insight beyond the Gleason Score alone, helping doctors personalize treatment decisions.
Source: Klein EA et al., European Urology (2014).
-
Should Gleason 6 Be Called Cancer? A Critical Review
Evaluates biological behavior of Gleason 6 tumors, concluding they lack metastatic potential and questioning whether the term “cancer” is appropriate.
Source: Ross HM et al., American Journal of Surgical Pathology (2012).
-
Prostate Cancer: Opinions Vary on Gleason Scores and Surgery
Interview with Dr. Bert Vorstman, MD, MS who argues that Gleason 6 lesions should not be labeled as “cancer” because they lack the capacity to spread or cause harm.
Source: Piana R (interviewing Vorstman B), ASCO Post (2016).
-
5 Challenges to Conventional Wisdom in Prostate Cancer
Dr. Bert Vorstman discusses why he believes Gleason 6 lacks the biological hallmarks of cancer and why over-diagnosis leads to overtreatment.
Source: Vorstman B, Medscape (2020).
-
Active Surveillance for Favorable-Risk Prostate Cancer: Ten-Year Outcomes
Finds extremely low risk of metastasis or death among men with Gleason 6 disease who were followed under active surveillance protocols.
Source: Tosoian JJ et al., European Urology (2020).